
The Science of Wound Healing: Supporting Each Phase for Optimal Recovery
Wound healing is a remarkable process that unfolds in four distinct but overlapping phases: hemostasis, inflammation, proliferation, and remodeling. Each phase plays a critical role in restoring tissue integrity after an injury, with specific cells, nutrients, and signals working in harmony to repair damage. The process begins with hemostasis, where bleeding is controlled, and a clot forms to protect the wound. This is followed by the inflammatory phase, during which the immune system clears debris and prepares the area for repair. Next, the proliferative phase builds a temporary framework of new blood vessels, collagen, and epithelial cells to rebuild the tissue. Finally, the remodeling phase strengthens and refines the new tissue, replacing the initial scaffold with mature collagen to restore durability and function. Understanding these phases and the nutrients that support them provides valuable insight into optimizing healing and addressing complications that may arise.

Phase 1: Stop the Bleeding (Hemostasis)
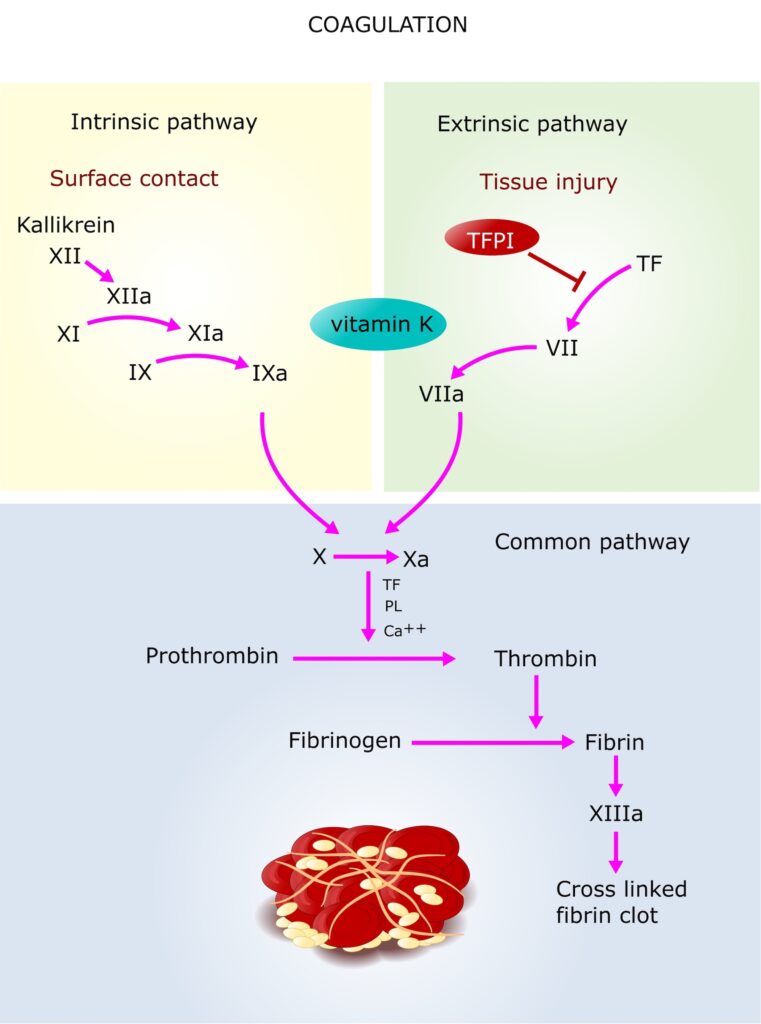
Overview: The body’s first response to injury is to stop the bleeding and stabilize the damaged tissue. This is called hemostasis. Depending on the type of tissue and how much blood flows to it, the healing process can vary. In areas with a high blood supply, the body uses clotting pathways to form a blood clot. In areas with low blood supply, like ligaments, tendons, or cartilage, healing relies on platelets coming into contact with connective tissue to start the repair process. PRP (Platelet-Rich Plasma) can help in both cases by boosting the body’s natural response.
Key Cellular Players:
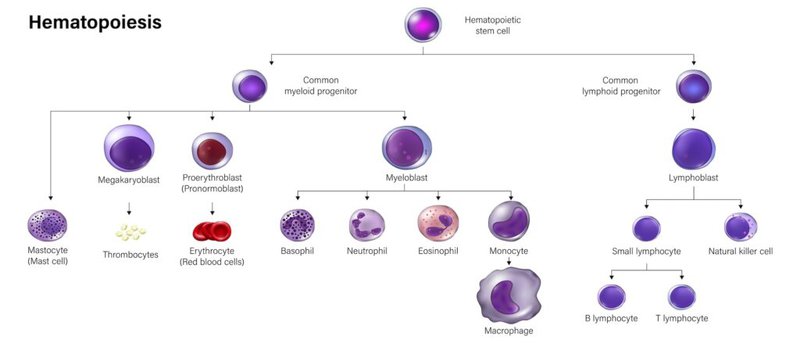
- Platelets: Gather at the injury site to create a temporary clot and release granules filled with clotting proteins, growth factors like PDGF, and signaling molecules that initiate the wound healing cascade.
- Endothelial Cells: Constrict to minimize blood loss and contribute to clot formation.
Healing in High-Blood-Supply Areas
- In areas with lots of blood flow, like muscles, the body uses the blood clotting pathway to heal. When a blood vessel is injured, it exposes connective tissue underneath. This triggers a chain reaction involving platelets and special proteins. Together, they form a clot to stop the bleeding and begin the healing process. Platelets also release growth factors that help repair the tissue.
Healing in Low-Blood-Supply Areas
- In tissues with little to no blood supply, like ligaments, tendons, or cartilage, the healing process relies on platelets coming into direct contact with connective tissue. When platelets touch these tissues, they become activated and release signals that start the repair process. These areas don’t have as many natural resources for healing, so the process can be slower.
How PRP Helps in Low-Blood-Supply Areas
Platelet-Rich Plasma (PRP) can be injected into low-blood-supply areas to speed up healing. PRP provides extra platelets, which release growth factors and mimic the body’s natural inflammatory process.
- Calcium-Activated PRP: Adding calcium to PRP can activate the platelets before they are injected. This mimics the way platelets work in high-blood-supply areas, creating a stronger inflammatory response. However, this may cause too much inflammation, especially in joints, tendons, or ligaments.
- Non-Calcium-Activated PRP: When PRP is not activated with calcium, it may lead to a more balanced, pro-reparative response without excessive inflammation. This approach is often preferred for delicate, low-blood-supply areas to avoid overstimulation.
Key Nutrients and Cofactors:
- Vitamin K: Essential for synthesizing clotting factors that are necessary to form a blood clot initiating the first stage of healing.
- Calcium: Required for platelet activation and stabilization of the coagulation cascade, ensuring clot formation.
- Iron: Oxygen as part of hemoglobin in red blood cells is necessary for platelet metabolism and activation. It supports tissue survival and cellular signaling at the wound site.
- Magnesium: Magnesium is involved in the energy metabolism required for platelet activation and granule release. Platelets require ATP to change shape, adhere to the injury site, and release the contents of their granules.
- Zinc: Zinc helps platelets stick together, supports clot formation, and repairs blood vessels. It’s crucial for stable clots and fast healing.
What Can Go Wrong:
- Vitamin K deficiency or clotting disorders can impair the synthesis of clotting factors, delaying hemostasis.
- Calcium depletion or poor vascular supply may hinder clot formation and platelet activation.
Phase 2: Inflammation
Overview: After the bleeding is controlled, the body shifts to cleaning up the damaged tissue and preparing for repair. This phase, known as inflammation, is triggered by signals from injured cells, bacteria, and platelets. These signals attract immune cells like neutrophils and macrophages, which play key roles in removing debris and fighting infection. Platelets, which helped form the initial clot, also express markers like P-selectin to recruit these immune cells. Supportive cells, such as mast cells and endothelial cells, regulate blood vessels to ensure immune cells can reach the injury site.
Key Cellular Players:
- Platelets: Signal for help from neutrophils and macrophages by releasing markers like P-selectin and other molecules that attract immune cells.
- Neutrophils: First to arrive at the injury. They clean up debris and kill bacteria by engulfing them and break down connective tissue to for cell migration to site of injury.
- Macrophages: Inflammatory macrophages, M1 macrophages, predominate this phase which produce pro-inflammatory signals to clear debris and fight infections.
- Mast Cells and Endothelial Cells: Help open blood vessels so immune cells and nutrients can reach the injury site.
Key Nutrients and Cofactors:
- Vitamin C: Vitamin C helps the body make signals that guide immune cells to injured areas. It keeps blood vessels healthy, boosts immune cell response to these signals, and protects the area from damage caused by too much stress or inflammation. This makes it easier for immune cells to find and fix the problem.
- Zinc: Zinc is important for your body to fight infection and heal wounds. It helps immune cells like neutrophils and macrophages work properly by guiding them to the injury, helping them clear out germs and damaged tissue, and controlling inflammation. Zinc also protects cells from stress, keeps blood vessels healthy, and supports the switch from cleaning up to starting the repair process.
- Omega-3 Fatty Acids: Helps balance inflammation, preventing excessive tissue damage and promoting a quicker resolution of the inflammatory phase.
- Selenium: Supports antioxidant production reducing oxidative stress, controlling inflammation, and protecting cells from damage.
- Glutamine: Glutamine gives immune cells like macrophages and neutrophils the energy they need to fight infection and clean up damaged tissue. It also helps keep the gut healthy, which can lower overall inflammation and support faster healing.
- Magnesium: Magnesium works to give immune cells the energy they need to work, controls signals that manage inflammation, and prevents the release of too many inflammatory signals. It also reduces oxidative stress and keeps blood flowing properly to the injury, helping the body heal without causing further harm.
- Vitamin D: Helps prevent chronic inflammation and supports the shift to the reparative phase.
- Arginine: Arginine helps the body make nitric oxide, which improves blood flow to the injury and helps immune cells move to where they’re needed. It also boosts macrophage activity, supporting faster healing.
What Can Go Wrong:
- Excessive Inflammation: Overactive immune responses can lead to prolonged or excessive inflammation, damaging healthy tissue around the injury.
- Insufficient Inflammation: If the immune system doesn’t respond strongly enough, debris and pathogens may not be cleared properly. This can result in delayed healing, infection, or the development of chronic wounds.
- Neutrophil Dysfunction: Overactive neutrophils can release too much ROS and proteases, causing unnecessary tissue damage. On the other hand, if neutrophils don’t function well, cleanup is incomplete, leaving obstacles for repair.
- Macrophage Imbalance: Failure to properly shift from M1 (pro-inflammatory) to M2 (pro-reparative) macrophages can prolong inflammation and prevent progression to the healing phases.
- Nutrient Deficiencies: Lack of key nutrients like zinc, vitamin C, or magnesium can weaken immune cell activity and prolong the inflammatory phase.
- Oxidative Stress Overload: Without enough antioxidants (like vitamin C or selenium), excessive ROS can damage both immune cells and healthy tissue, leading to stalled healing and chronic inflammation.
- Vascular Issues: Poor blood flow to the injury site can limit oxygen, nutrients, and immune cell delivery, slowing the inflammatory process and impairing repair.
- Systemic Conditions: Chronic conditions like diabetes or autoimmune disorders can disrupt the inflammatory phase, either by dampening immune responses or causing persistent, harmful inflammation.
Phase 3: Repair (Proliferation)
Overview: The proliferative phase starts when the body moves from cleaning up the injury to repairing it. This happens as inflammation slows down, and macrophages switch from their inflammatory role (M1) to a repair-focused role (M2). As neutrophils complete their role, they are engulfed by macrophages helping the tissue switch from inflammation to repair. These reparative macrophages release growth factors like VEGF and TGF-β, which signal other cells to start rebuilding. Fibroblasts make collagen to form a temporary structure, endothelial cells create new blood vessels, and keratinocytes restore the skin barrier to protect the wound. This phase sets the foundation for healing and tissue repair.
Key Cellular Players:
- Platelets: Continue to release growth factors such as PDGF and VEGF, which promote fibroblast activity, angiogenesis, and tissue repair. Play a role in guiding cell migration and maintaining a supportive microenvironment for healing.
- Fibroblasts: Fibroblasts make collagen (type III) to help form a structure that other cells can use to repair the wound. They also turn into special cells called myofibroblasts, which pull the wound edges together to help it close.
- Endothelial Cells: Form new blood vessels (angiogenesis) in response to growth factors like VEGF, improving oxygen and nutrient delivery to the wound site.
- Keratinocytes: Migrate across the wound bed to restore the epithelial barrier, protecting the area from further injury or infection.
- Macrophages (M2): Shift from an inflammatory to a reparative role, releasing growth factors such as TGF-β and FGF to stimulate fibroblasts and enhance angiogenesis.
Key Nutrients and Cofactors:
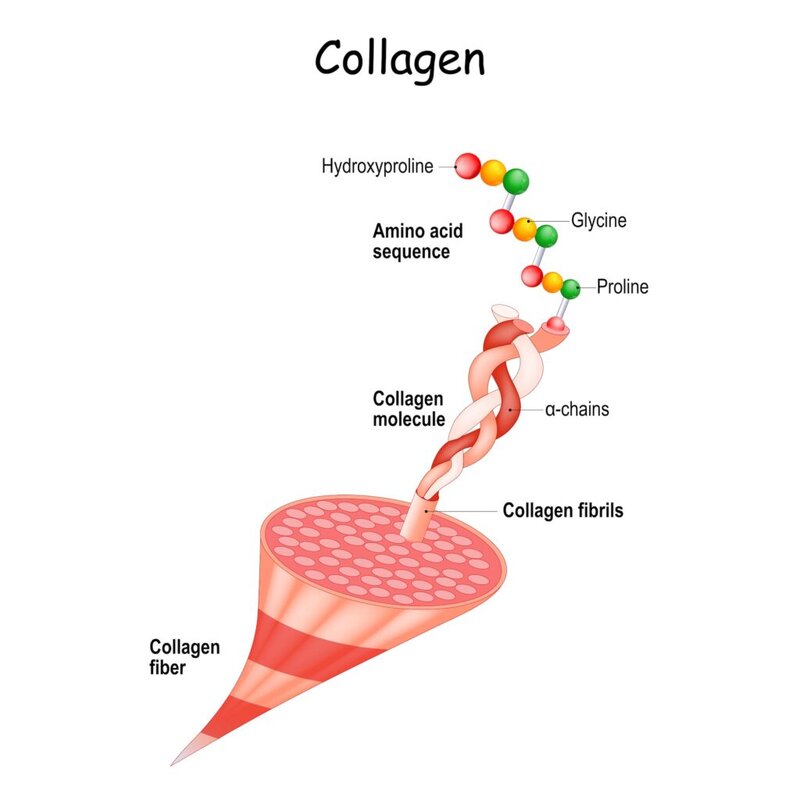
- Vitamin C: Critical for collagen stabilization through the hydroxylation of proline and lysine.
- Vitamin A: Supports epithelial cell growth and differentiation, essential for wound closure and barrier restoration.
- Vitamin D: Modulates immune responses and promotes calcium absorption, aiding tissue repair and regeneration.
- Copper: Required for lysyl oxidase, which strengthens and cross-links collagen fibers.
- Magnesium: Activates enzymes necessary for collagen synthesis and supports DNA and protein production in fibroblasts and endothelial cells.
- Calcium and Phosphorus: Essential for mineralizing new tissue and maintaining structural integrity during the repair process.
- Sulfur: Necessary for synthesizing disulfide bonds in collagen and other structural proteins.
- Silicon: Plays a role in collagen synthesis and maintaining skin and connective tissue strength.
- Amino Acids: Glycine, Proline, and Hydroxyproline: Form the backbone of collagen for strength and flexibility. Lysine: Supports enzymatic cross-linking for tensile strength. Arginine: Promotes nitric oxide production, improving blood flow and oxygen delivery.
- Iron: Functions as a cofactor for enzymes involved in collagen stabilization.
- Glycosaminoglycans (GAGs): Include Hyaluronic Acid (HA), Chondroitin Sulfate, Dermatan Sulfate, and Heparan Sulfate. These molecules retain moisture, provide structural support to the extracellular matrix, and facilitate cell migration and attachment.
- Glutathione: Protects cells from oxidative damage and supports the activity of fibroblasts and other repair cells.
- Omega-3 Fatty Acids: Reduce inflammation and support cellular membrane repair, promoting a balanced healing environment.
What Can Go Wrong:
- Insufficient Collagen Production: Without enough buidling blocks and cofactors like vitamin C, copper, or amino acids, fibroblasts cannot produce sufficient collagen. This leads to weak or incomplete tissue repair, increasing the risk of wound reopening or poor structural integrity.
- Impaired Angiogenesis: A lack of key nutrients like iron or signals like VEGF can prevent new blood vessels from forming. This limits oxygen and nutrient delivery to the wound, slowing healing and increasing the risk of chronic wounds.
- Excessive Scar Tissue Formation: If fibroblasts produce too much collagen or matrix remodeling is delayed, it can result in fibrosis or excessive scarring, which may reduce tissue flexibility and function.
- Delayed Keratinocyte Migration: Without proper keratinocyte activity, the wound bed cannot close effectively. This leaves the wound exposed to infection and slows the repair process.
- Chronic Wound Development: Failure to fully transition from the inflammatory phase can leave wounds stuck in a cycle of inflammation, delaying the start of tissue repair.
- Poor Hydration or ECM Support: A lack of hyaluronic acid or GAGs can result in a dry wound environment, reducing cell migration and attachment necessary for tissue repair.
- Systemic Factors: Chronic conditions like diabetes or malnutrition can impair fibroblast function, angiogenesis, and collagen synthesis, further delaying wound healing.
Phase 4: Maturation (Remodeling)

Overview: The remodeling phase is the final stage of wound healing, beginning weeks after the injury and lasting for months or even years. During this phase, the temporary extracellular matrix (ECM) laid down in the proliferative phase is replaced with stronger, more organized tissue. Type III collagen is gradually replaced by Type I collagen, which provides greater tensile strength. Cells involved in earlier phases, such as fibroblasts and macrophages, reduce their activity or undergo apoptosis as the tissue reaches maturity. Mechanical stress helps align collagen fibers along tension lines, optimizing tissue strength and functionality.
Key Cellular Players:
- Fibroblasts and Myofibroblasts: Fibroblasts continue to remodel the ECM by replacing Type III collagen with Type I collagen. Myofibroblasts help contract the wound edges and promote alignment of collagen fibers.
- Macrophages (M2): Clear apoptotic cells and remaining debris. Continue to secrete growth factors like TGF-β to regulate fibroblast activity and collagen deposition.
- Endothelial Cells: Newly formed capillaries from the proliferative phase are pruned to match the tissue’s metabolic demands, leaving behind a mature vascular network.
- Matrix Metalloproteinases (MMPs): Enzymes that break down excess or improperly laid ECM components to refine and optimize the tissue structure.
Key Nutrients and Cofactors:
- Vitamin C: Critical for stabilizing and cross-linking collagen through the hydroxylation of proline and lysine.
- Amino Acids: Glycine, Proline, and Hydroxyproline are essential for replacing Type III collagen with stronger Type I collagen. Lysine supports collagen cross-linking, contributing to tissue tensile strength. Arginine enhances blood flow and nutrient delivery through nitric oxide production.
- Copper: Cofactor for lysyl oxidase, an enzyme required for collagen cross-linking and tissue strength.
- Zinc: Regulates MMP activity to balance collagen degradation and deposition during remodeling.
- Sulfur: Supports the formation of disulfide bonds, stabilizing collagen and other structural proteins.
- Glutathione: Protects cells and collagen from oxidative damage, ensuring ECM stability.
- Magnesium: Supports ATP production and enzymatic processes essential for fibroblast activity and collagen turnover.
- Omega-3 Fatty Acids: Reduces residual inflammation, stabilizes cell membranes, and improves tissue quality.
- Calcium and Phosphorus: Contribute to the mineralization of bone and cartilage for ECM strength and stability.
- Vitamin A: Promotes epithelial regeneration and fibroblast activity for proper tissue remodeling.
- Vitamin D: Modulates immune activity to resolve lingering inflammation and supports calcium metabolism.
- Silicon: Enhances collagen synthesis, cross-linking, and ECM integrity.
- Glycosaminoglycans (GAGs): Includes hyaluronic acid, chondroitin sulfate, and heparan sulfate. Maintains hydration, provides structural support, and aids in fibroblast activity and collagen alignment.
What Can Go Wrong:
- Weak Collagen Structure: Insufficient building blocks and cofactors for collagen production like vitamin C, copper, or amino acids can result in poorly cross-linked collagen, leading to weak and fragile tissue that is prone to reinjury.
- Excessive Scar Tissue (Fibrosis): Overactive fibroblasts or reduced matrix metalloproteinase (MMP) activity can lead to excessive collagen deposition. This results in stiff, inflexible scar tissue that can impair function, especially in joints and tendons.
- Delayed or Improper Remodeling: Lack of mechanical stress or poor collagen alignment prevents optimal tissue strength and functionality. Inadequate levels of zinc or magnesium can disrupt the balance between collagen synthesis and degradation.
- Chronic Wounds: Failure to resolve earlier inflammatory signals can leave wounds in a persistent inflammatory state, preventing proper remodeling and wound closure.
- Impaired Angiogenesis Pruning: Poor vascular remodeling due to insufficient signals like VEGF or hypoxia regulation can result in an overabundance or disorganized blood vessels, reducing tissue efficiency and durability.
- Oxidative Stress: A lack of antioxidants like glutathione can cause oxidative damage to newly formed collagen and ECM components, weakening the repaired tissue.
- Poor ECM Hydration: A deficiency in hyaluronic acid or other glycosaminoglycans (GAGs) can result in a dry, brittle ECM, reducing flexibility and impeding cell migration.
- Mineral Deficiencies: Low levels of calcium, phosphorus, or silicon can impair mineralization in bones and cartilage, compromising the structural stability of the ECM.
- Systemic Factors: Conditions like diabetes or malnutrition can slow fibroblast activity, reduce collagen production, and impair overall remodeling. Chronic inflammation from autoimmune disorders or unresolved infections can disrupt the balance needed for proper tissue maturation.
Wound healing is a natural process that the body is well-equipped to handle, provided it has the necessary support. Proper nutrition and exercise lay the foundation for effective healing by supplying essential nutrients and improving circulation and tissue strength. Regenerative medicine, such as advanced orthobiologics (PRP, micronized fat, bone marrow aspiration concentrate, and donor tissue), can complement these efforts by enhancing the body’s natural repair mechanisms with targeted growth factors and cellular support. By integrating these advanced therapies with strong health foundations, we can optimize the healing process, improve outcomes, and build a more resilient body capable of recovering quickly and effectively.